

Can You Take Creatine While Pregnant? What the Research Actually Says

Written by Stephanie Castanedo, ND Board-Certified Naturopathic Doctor & Clinical Nutritionist.
Key Takeaways
Creatine is well studied and generally safe in healthy non-pregnant adults, but human pregnancy data is still limited.
Major reviews conclude that caution is warranted, and no completed randomized trial in pregnant humans exists yet.
Most pregnancy-related benefits, such as fetal neuroprotection, come from animal studies rather than proven human outcomes.
Creatine does cross the placenta, and maternal creatine demand rises in pregnancy, which is why researchers are studying it.
The right move is a personal decision made with an OB or a certified prenatal nutritionist, not a blanket yes or no.
Introduction
Creatine is one of the most popular and most heavily researched supplements on the market, so it is no surprise that pregnant people want to know whether it belongs in a prenatal routine. The problem is that the advice online swings wildly. One article says it is totally fine, and the next says to stop immediately. For a parent who is active, follows a vegetarian or vegan diet, or has already been taking creatine for years, that whiplash is stressful and unhelpful.
Wanting steady energy during pregnancy does not make anyone a careless parent. It makes them a normal one. This guide takes a different approach from the usual one-line answer. It lays out what the evidence actually shows, separates what is proven from what is only promising, and offers a simple framework to help decide what fits a specific situation. Along the way it also flags the dosing details and the diet-first option that most quick answers leave out, plus the questions worth bringing to a professional. The goal is clarity, not hype and not fear.
What Is Creatine, and Why Are Pregnant People Asking About It?
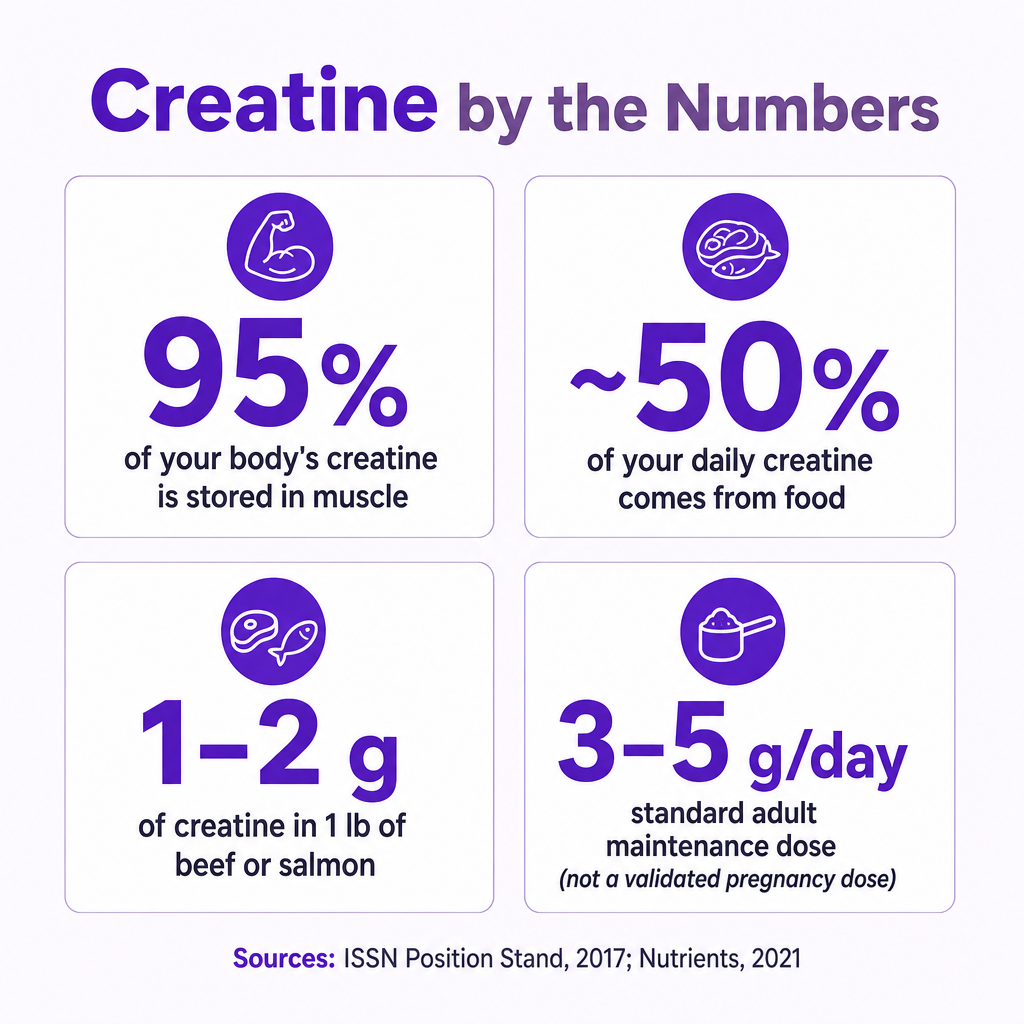
Creatine is a compound derived from amino acids that the body uses to produce quick bursts of energy. Roughly 95% of the body's creatine is stored in skeletal muscle, where it helps cells rapidly regenerate ATP, the molecule that powers short, intense effort, according to the International Society of Sports Nutrition Position Stand (Kreider et al., 2017).
The body gets creatine from two places. About half of the daily requirement comes from diet, mainly red meat and seafood, and the body synthesizes the rest on its own, per the ISSN Position Stand (2017).
So why does pregnancy raise the question at all? A few reasons converge:
Pregnancy is a high-energy-demand state, and maternal creatine demand rises across gestation, as described by Dickinson et al., BMC Pregnancy and Childbirth (2014).
Creatine's popularity in mainstream fitness has grown, so more people entering pregnancy are already using it.
Vegetarians and vegans take in less dietary creatine, which is one reason they often ask whether they need more, as vegetarians have reduced baseline creatine stores compared with omnivores, per Kaviani et al., Nutrients (2020).
There is also a physiological reason the topic keeps surfacing. Because the developing fetus relies on creatine delivered across the placenta and the mother's own stores are drawn on to support that demand, the pregnancy body is working harder to keep creatine balanced than it does at baseline, per Dickinson et al. (2014). That biology is precisely why researchers find the question worth studying, and it is also why a personalized answer beats a generic one.
These are exactly the "does this apply to me?" questions that a certified prenatal nutritionist is trained to answer.
Is Creatine Safe During Pregnancy? The Honest Answer
Here is the direct answer first. In healthy non-pregnant adults, creatine taken by mouth at recommended doses is considered generally safe, possibly for up to five years of use, according to the Mayo Clinic (2026). That is the strong, well-established part of the picture.
Creatine and pregnancy: what the evidence actually shows.
The pregnancy caveat is where honesty matters. Leading expert reviews conclude that because studies in pregnant humans are limited, "caution should be exercised when recommending use during human pregnancy," per Creatine in Health and Disease, Nutrients (2021). The same review notes there is no evidence that creatine poses a risk to women of reproductive age, while stressing that additional safety and tolerability studies in pregnant women are still needed.
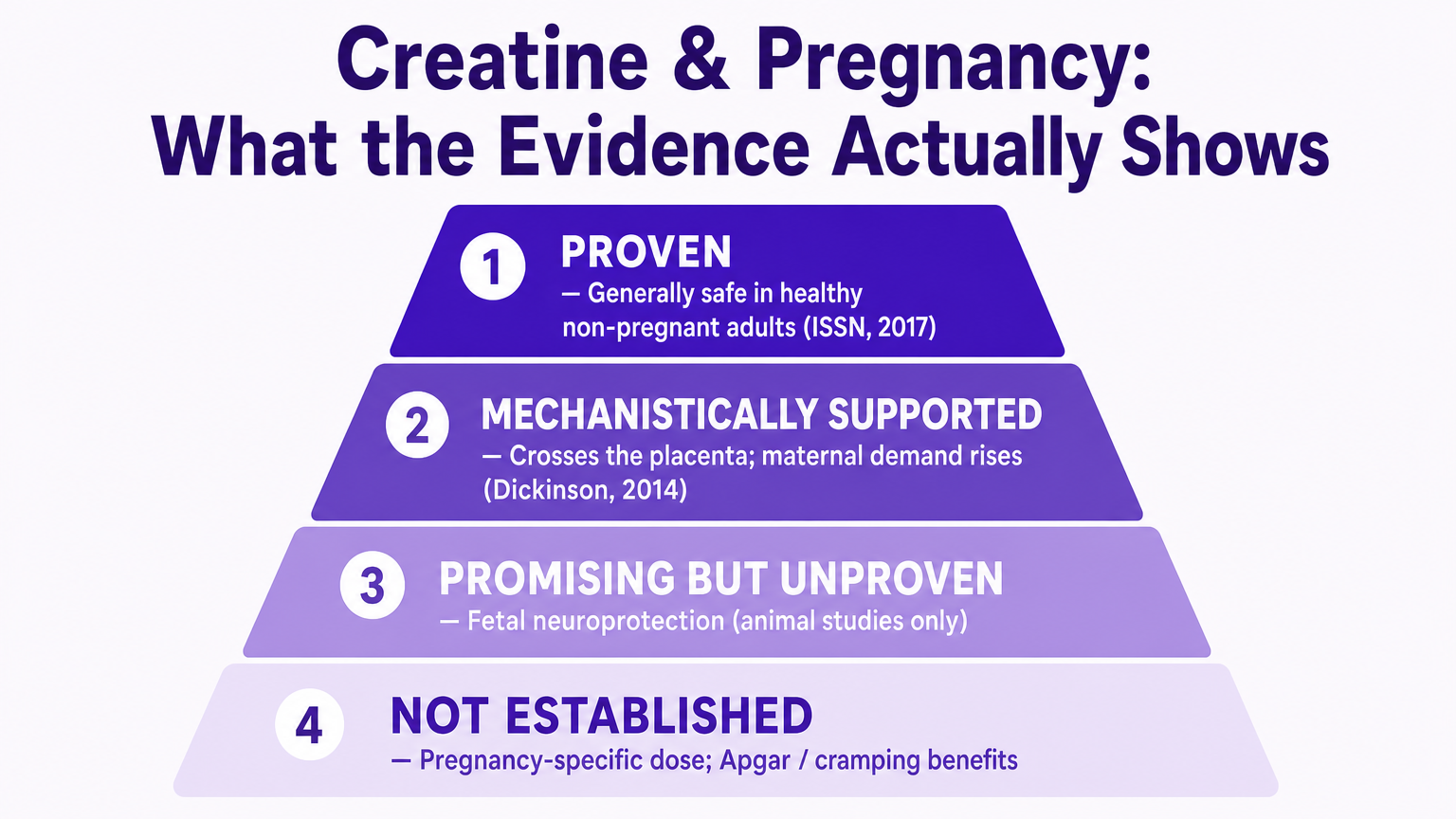
The reason sources disagree is that they collapse very different tiers of evidence into a single verdict. Here is the synthesis most articles skip:
Proven: General safety and benefit in healthy adults, per the ISSN Position Stand (2017).
Mechanistically supported: Creatine crosses the placenta, and maternal demand rises during pregnancy, per Dickinson et al. (2014).
Promising but unproven in humans: Fetal neuroprotection, which so far rests on animal models.
Not established: Specific pregnancy dosing and outcomes such as improved Apgar scores or reduced cramping that some websites claim.
One more caution belongs here. No completed randomized controlled trial of creatine in human pregnancy is documented in the peer-reviewed literature, per Dickinson et al. (2014). Be skeptical of articles that cite suspiciously specific recent trials with exact participant counts, because several of those references do not appear to hold up. An honest "we do not fully know yet" is more trustworthy than false certainty.
This tiered view also explains why blanket claims in either direction miss the mark. A source that says creatine is simply safe in pregnancy is borrowing confidence from the adult research and applying it where it has not been tested. A source that says to avoid it entirely is treating "not yet proven" as if it meant "shown to be harmful," which the evidence does not support either. The measured reading is that there is no documented risk signal in reproductive-age women, alongside a genuine gap in pregnancy-specific human data, per Creatine in Health and Disease, Nutrients (2021). Holding both of those facts at once is the whole point.
What Does the Research Actually Show?
The evidence base is real, but it is uneven. Sorting it by strength is the clearest way to understand it.
Where the Evidence Is Strong: Healthy Adults
For the general adult population, creatine monohydrate is the most studied form and is considered safe and effective, according to the ISSN Position Stand (2017). This is the part of the conversation with decades of data behind it. Commonly raised concerns about kidney harm are not supported in healthy users at recommended doses, though research in people who already have kidney disease is limited, per the Mayo Clinic (2026). The key limitation is simple to state: this strong safety record was built in non-pregnant adults, so it cannot be stretched to cover pregnancy without more direct evidence.
Where It Is Still Early: Human Pregnancy
Pregnancy research is far less developed:
Animal studies, notably in the spiny mouse, show that maternal creatine can protect the newborn brain, diaphragm, and kidney from birth-asphyxia injury and can improve survival, with no obvious harm to mother or pup, per Dickinson et al. (2014). These are animal findings, not confirmed human outcomes.
The leading human work is observational. The de Guingand prospective cohort in low-risk pregnant women in Australia measured how maternal creatine changes across pregnancy and how it relates to diet, per de Guingand et al., American Journal of Clinical Nutrition (2023). It lays groundwork for future trials but is not itself a completed interventional trial.
The bottom line is a promising biological mechanism paired with incomplete human safety and efficacy data.
Potential Benefits and Risks: What to Weigh
A balanced look means naming both sides plainly and labeling how solid each point is.
Potential upside (theoretical or early): Creatine supports cellular energy metabolism, is actively transported across the placenta, and has been studied for fetal neuroprotection in animal models, per Dickinson et al. (2014). None of these upsides is yet proven to benefit healthy human pregnancies.
Potential concern (hydration and existing conditions): Adequate hydration matters, and people with pre-existing kidney disease should consult a clinician before use, per the Mayo Clinic (2026).
Potential concern (product quality): The FDA does not approve dietary supplements for safety or effectiveness before they are marketed, so quality varies by manufacturer, per the U.S. FDA (Dietary Supplements).
Some groups have more reason to be careful. Anyone with kidney or liver conditions, a history of preeclampsia or gestational hypertension, or who takes medications that affect the kidneys should treat supplementation as a conversation with a provider rather than a personal experiment.
It is worth keeping the placental point in perspective too. The fact that creatine crosses the placenta is often presented as a benefit, but on its own it only describes a transport mechanism, per Dickinson et al. (2014). It does not prove that a healthy pregnancy needs supplemental creatine or that adding more improves outcomes. Weighing benefits and risks here means resisting the urge to read a proven mechanism as a proven result.
How Much Creatine Is Studied, and What About Diet First?
Dosing is where a lot of confusion creeps in, so precision helps.
Creatine Statistics
The established adult maintenance dose is 3 to 5 grams per day of creatine monohydrate, sometimes preceded by an optional loading phase of about 0.3 grams per kilogram per day for 5 to 7 days, per the ISSN Position Stand (2017).
The important nuance is that these are general-adult figures. They are not a validated pregnancy prescription, and no reliable source establishes a pregnancy-specific dose.
Food is a reasonable starting point for many people. A pound of uncooked beef or salmon provides roughly 1 to 2 grams of creatine, and omnivore diets typically supply about 0.75 to 1.5 grams per day, per the ISSN Position Stand (2017) and Creatine in Health and Disease, Nutrients (2021). Between diet and the body's own synthesis, many people already meet their needs.
If a supplement is the chosen route, the practical guidance is to select a creatine monohydrate product that follows good manufacturing practices and carries independent third-party verification, such as the U.S. Pharmacopeia (USP) Dietary Supplement Verification Program. Third-party testing matters more than usual during pregnancy because, as noted above, dietary supplements are not reviewed by the FDA for safety or effectiveness before they reach the shelf, per the U.S. FDA (Dietary Supplements). A verified product reduces the risk of contaminants or inaccurate labeling, which is one variable worth removing from an already uncertain decision.
How Should You Decide? A Simple Framework
There is no universal answer, so the useful thing is a repeatable way to reach a personal one. The reason a framework helps is that the science does not point to one right choice for everyone. It points to general adult safety, a real but early pregnancy picture, and a set of individual factors that only the person and their provider can weigh together, per Creatine in Health and Disease, Nutrients (2021). Work through these steps:
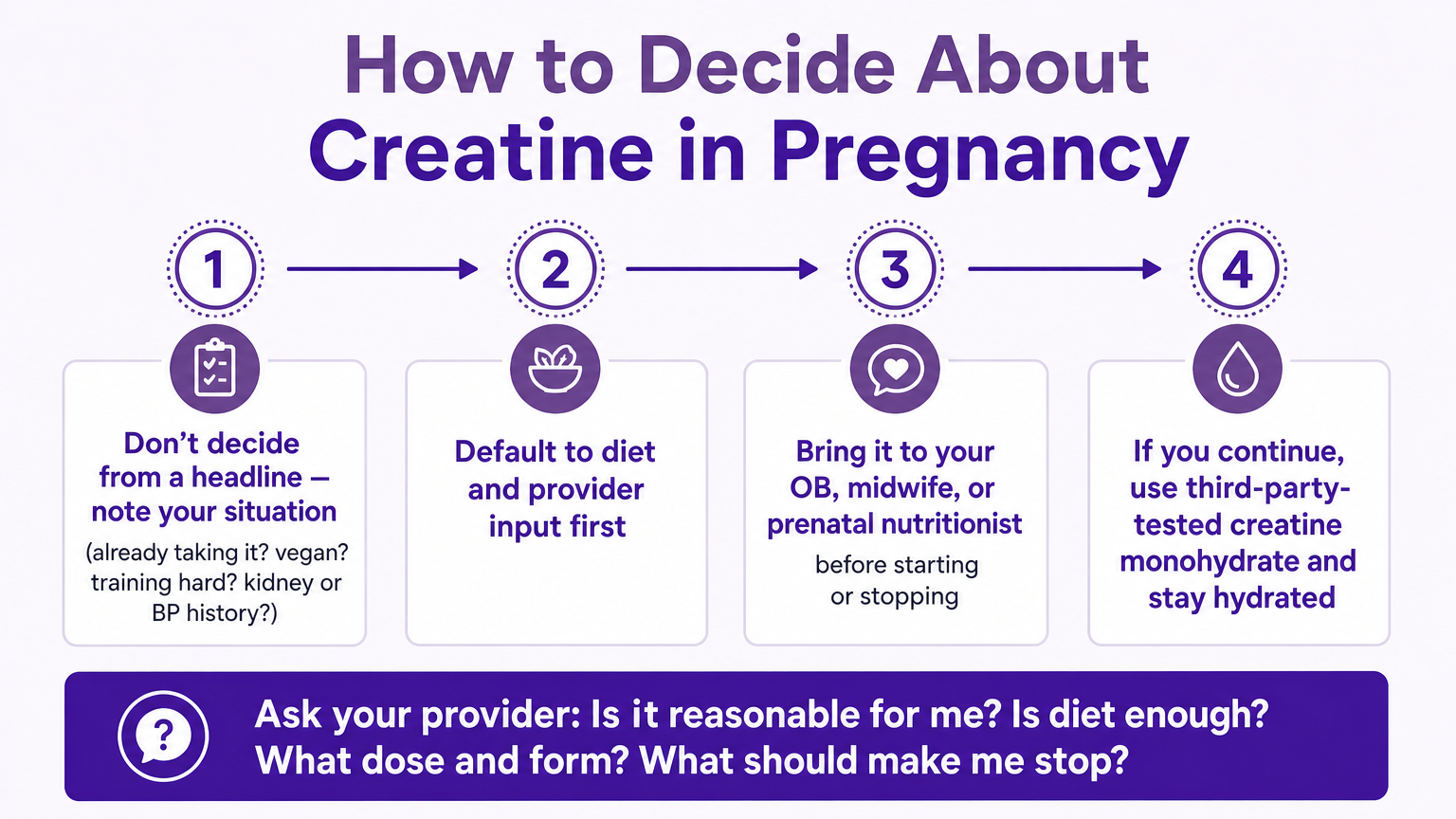
How to decide about creatine in pregnancy?
Step 1: Do not decide from a headline. Write down the specific situation, including whether creatine is already part of the routine, whether the diet is vegetarian or vegan, how hard the training is, and any kidney or blood-pressure history.
Step 2: Default to diet and provider input first. There is rarely urgency to start a brand-new supplement mid-pregnancy, so food and a professional opinion come before a purchase.
Step 3: Bring it to a professional. Raise the question with an OB, midwife, or certified prenatal nutritionist before starting or stopping.
Step 4: If continuing or starting, keep it standard. Use a third-party-tested creatine monohydrate at standard doses and stay well hydrated.
To make that conversation productive, bring a short list of questions:
Given my health history, is supplementation reasonable for me?
Is diet alone enough to cover my needs?
What dose and form would you recommend?
What signs or symptoms should make me stop?
Answers to those questions turn a vague internet debate into a plan that fits one specific pregnancy. A provider can weigh a real health history against the current evidence in a way no article can. This is exactly the kind of personalized, non-clinical guidance MissPoppins is built for, connecting parents with certified prenatal nutritionists online, often the same day, so the decision does not have to happen alone at 2am.
Frequently Asked Questions
Can you take creatine monohydrate while pregnant?
Monohydrate is the most researched form, but because human pregnancy data is limited, discuss use with a provider before taking it.
Does creatine cross the placenta?
Yes. Creatine is actively transported across the placenta, with transfer capacity present from at least 13 weeks of gestation, per Dickinson et al. (2014).
Should I stop taking creatine if I find out I'm pregnant?
There is no evidence it is harmful, but the cautious, evidence-based step is to pause and confirm with an OB or prenatal nutritionist.
What are the benefits of creatine while pregnant?
Proposed benefits like fetal neuroprotection come mainly from animal studies and are not yet proven in humans.
Can you take creatine while breastfeeding?
Human data is limited, so as with pregnancy, prioritize diet and check with a provider before supplementing.
Can you take creatine while trying to conceive?
Current reviews find no evidence that it harms women of reproductive age, but discuss it with a provider, especially during fertility treatment.
Conclusion: The Bottom Line
The honest verdict is straightforward. Creatine is generally safe for healthy adults, but its use in pregnancy is not yet proven, which makes it a personal, provider-guided decision rather than a simple yes or no. Wanting more energy and doing careful homework does not make anyone a bad parent. The calm, evidence-based move is to prioritize diet first and bring the question to an expert who knows the full health picture. That way the choice fits the person making it, not a headline.