

Can You Breastfeed Without Giving Birth? How to Induce Lactation as a Non-Gestational Parent

Written by Abigail Miles, a lactation consultant with 15+ years supporting non-gestational parents through induced lactation.
Breastfeeding is often described as one of the most intimate experiences between parent and child. But what if you didn't carry the pregnancy? Whether you're an adoptive parent, an intended parent through surrogacy or adoption, a same-sex partner who didn't give birth, or a transgender parent, induced lactation may make breastfeeding possible and the evidence is more encouraging than most people realize.
This guide breaks down the science behind induced lactation, the main protocols available, a realistic week-by-week timeline, and how to find the right professional support. Our goal is to give non-gestational parents the information they need to make a confident, informed decision about whether induced lactation is right for their family.
Key Takeaways
Induced lactation allows non-gestational parents (including adoptive, surrogacy, same-sex, and transgender parents) to breastfeed.
The Newman-Goldfarb protocol and pumping-only approaches offer flexible options based on your timeline.
A 2025 study found 87.5% of non-gestational mothers successfully initiated milk production.
A supplemental nursing system lets your baby nurse at the breast while building your supply.
Working with an IBCLC experienced in induced lactation significantly improves outcomes.
What Is Induced Lactation?
Induced lactation is the process of stimulating breast milk production in someone who has not been pregnant or given birth. It is distinct from relactation, which refers to restarting milk production after a person has previously breastfed.
The practice is relevant to a wide range of family structures. Adoptive parents, intended parents through surrogacy, same-sex couples where one partner did not carry the pregnancy, and transgender parents may all be candidates for induced lactation. According to La Leche League International (LLLI), "for most parents with adequate information and support, milk production begins within 6-8 weeks of beginning the process."
How realistic is success? A 2025 study published in PMC found that 87.5% of non-gestational mothers successfully initiated milk production when following established protocols. That figure is far more encouraging than the cautious "might be possible" language found in many clinical summaries.
Outcomes do vary. Some parents achieve a full milk supply; many achieve a partial supply that they supplement with formula or donor milk. Both outcomes are meaningful. Per WHO breastfeeding recommendations, any amount of breastmilk provides immunological benefits and supports the bonding process between parent and child. For more on breast milk safety and storage, MissPoppins has additional resources.
How Does the Body Produce Milk Without Pregnancy?
During pregnancy, rising levels of estrogen and progesterone prepare breast tissue for milk production. This process is explained in more detail in MissPoppins' guide on how lactation normally begins during pregnancy. After birth, the drop in these hormones allows prolactin, the hormone that drives actual milk synthesis, to take over. Prolactin production is triggered by nipple stimulation.
Here is the key insight: prolactin responds to breast stimulation regardless of pregnancy history. The body can be prompted to produce milk through consistent, repeated nipple stimulation such as pumping or hand expression. This is why breast stimulation is the foundation of every induced lactation protocol, with or without medication.
Medications used in some protocols work by mimicking the hormonal environment of pregnancy. Combined oral contraceptives supply estrogen and progesterone to prepare breast tissue, while metoclopramide or domperidone (not available in the US) raises prolactin levels. When the contraceptive is stopped and pumping begins, the hormonal shift mirrors what happens after birth.
Oxytocin, the hormone responsible for milk ejection (also called let-down), is triggered by skin-to-skin contact and emotional bonding with the baby. Research from the American Academy of Pediatrics confirms that skin-to-skin contact improves milk production and bonding. This means that the act of holding and nursing a baby actively supports the milk production process.
Three Approaches to Inducing Lactation
There is no single protocol for induced lactation. The right approach depends on your timeline, medical history, and personal preferences. Below are the three most widely referenced methods.
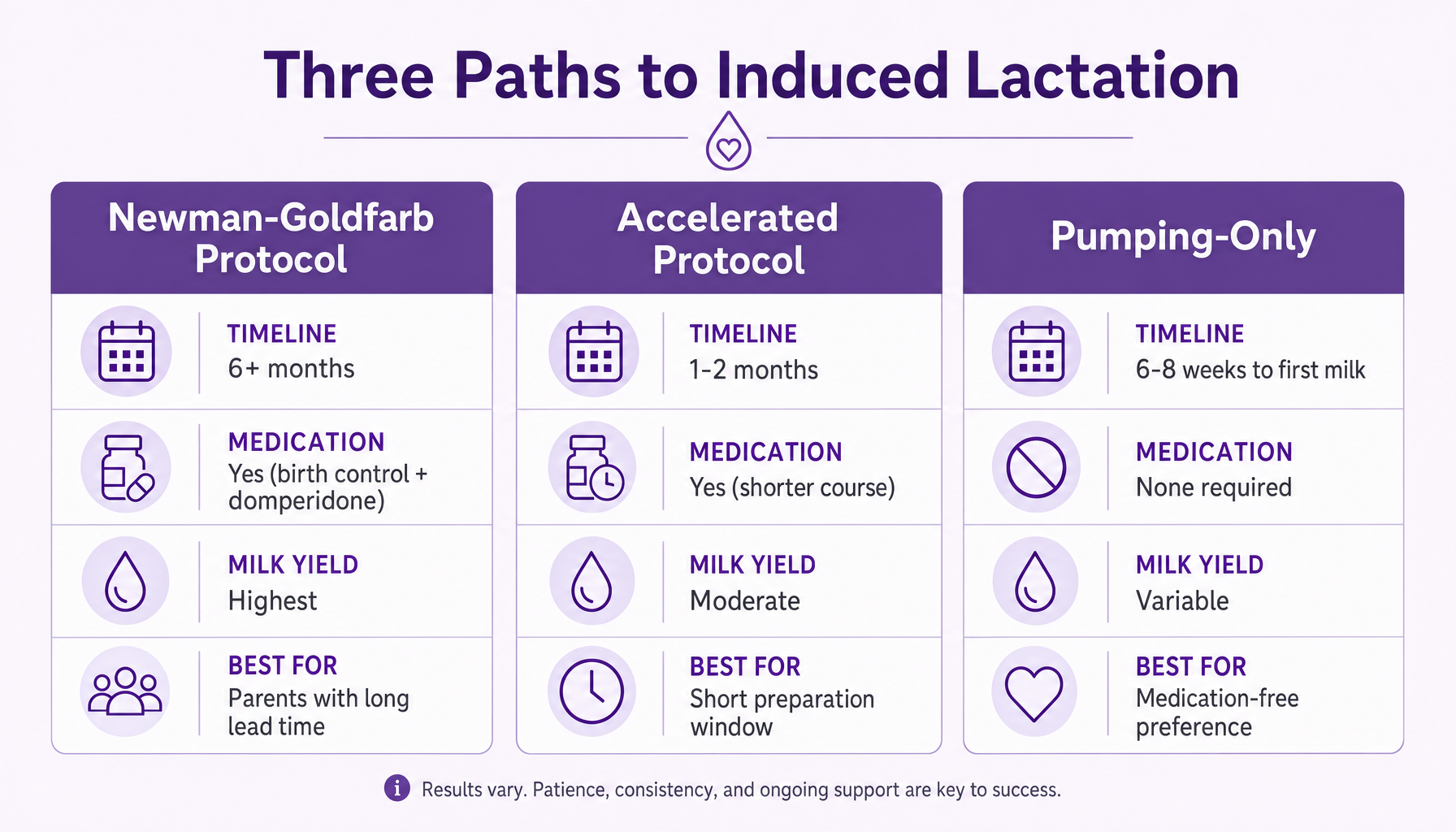
Three Paths to Induced Lactation
The Newman-Goldfarb Protocol (6+ Months) *domperidone (not available in the US)
Developed by Dr. Jack Newman and Lenore Goldfarb, PhD, IBCLC, this is the most comprehensive protocol and typically produces the highest milk yield. It involves three phases:
Phase 1, Hormonal Preparation: Take a combined oral contraceptive pill (monophasic, active pills only, no sugar pills) along with domperidone 20 mg four times daily (or another medication that increases prolactin. This step always requires medical guidance. It's not one size fits all.) Begin this phase at least six months before the baby is expected to arrive. According to the Canadian Breastfeeding Foundation, "the longer the mother can be on her particular protocol, the more milk she will end up with."
Phase 2, Transition to Pumping: Stop the birth control pill six to eight weeks before the baby arrives. Continue prolactin increasing medication. Begin pumping to signal the body to start producing milk.
Phase 3, Breastfeeding with Supplementation: Once the baby arrives, breastfeed at the breast using a supplemental nursing system (SNS) while continuing to pump between feeds to build supply.
An important note for parents in the United States: domperidone is not FDA-approved. The FDA issued a warning against its use in 2004 due to potential cardiac risks in certain individuals. It is available in Canada, the United Kingdom, Australia, and most other countries. US-based parents may access it through compounding pharmacies or with physician guidance, but sourcing it online without medical supervision is not safe. Domperidone carries cardiac risks that require screening before use. Discuss alternatives and access options with a healthcare provider familiar with induced lactation.
The Accelerated Protocol (1-2 Months)
For parents with a shorter preparation window, such as an unexpected adoption match or a compressed surrogacy timeline, the Accelerated Protocol condenses the hormonal preparation phase.
Take a combined oral contraceptive plus the prolactin increasing medication for 30 to 60 days.
Stop the birth control pill when significant breast changes occur (tenderness, fullness).
Begin pumping immediately.
Expected milk volume is typically lower than with the Regular Protocol, but any breastfeeding provides bonding and immunological value. As Goldfarb notes, "There is more to breastfeeding than breastmilk."
Pumping-Only (No Medication)
For parents who prefer a medication-free approach or cannot access the necessary prescriptions, breast stimulation alone can induce lactation. A scoping review published on ResearchGate (2020) confirmed that "pharmacological methods were not always used to produce milk, although breast stimulation was essential."
This approach involves:
Pumping or hand expression every two to three hours, including at least once overnight
Gradually increasing pump session duration as the body responds
Optionally adding galactogogues (herbal supplements for postpartum care such as Moringa or Milk thistle), though evidence for their effectiveness is limited
Milk production typically begins within six to eight weeks with consistent stimulation. Expected volume may be lower than with medication-assisted protocols, but any amount of breastmilk delivers antibodies, supports healthy gut flora, and reinforces the parent-child bond.
What to Expect: A Realistic Timeline
One of the biggest gaps in existing information about induced lactation is a clear, week-by-week picture of what the process actually looks like. Here is a general framework, though individual experiences vary based on protocol, consistency, and physiology.
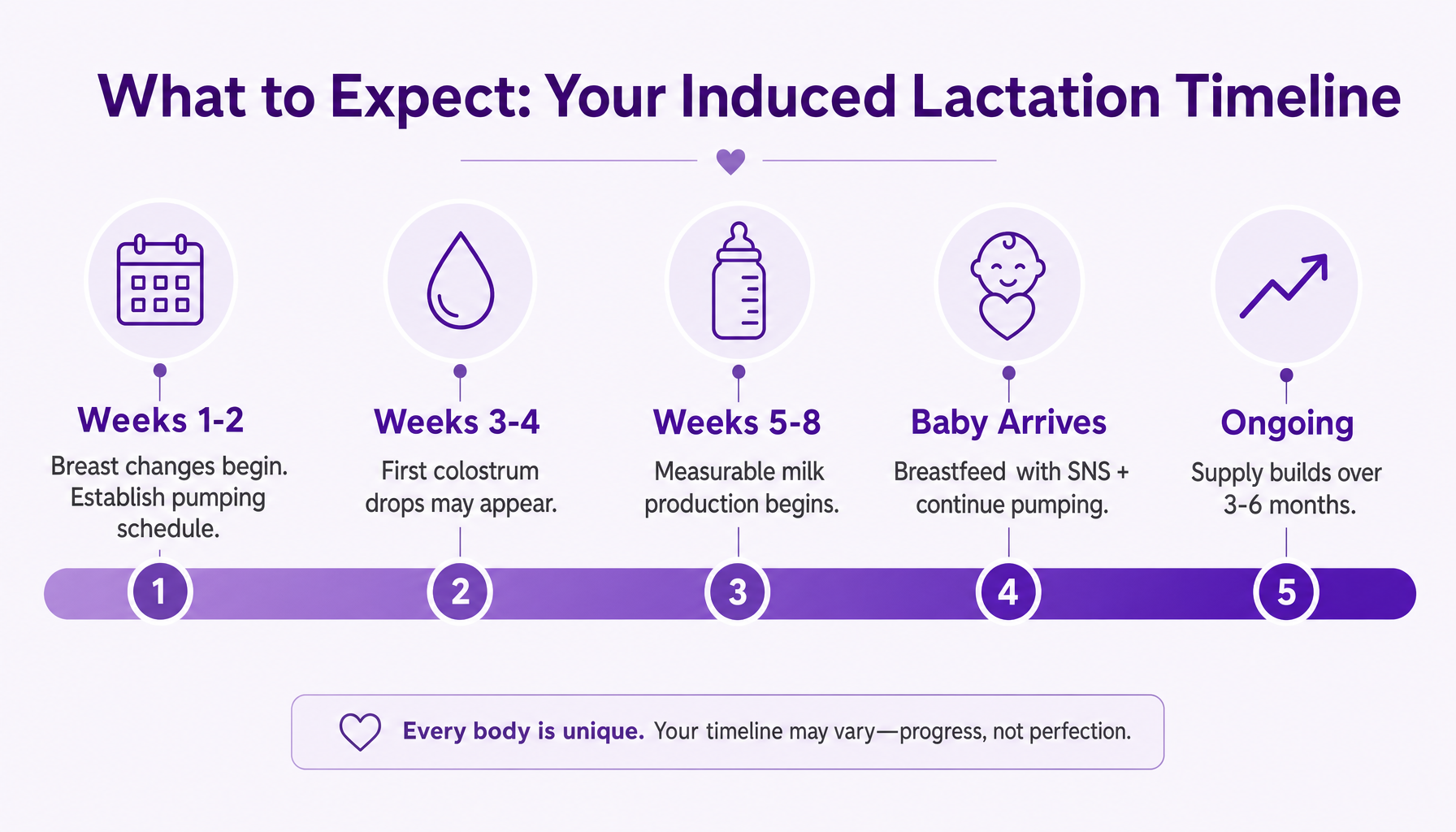
What to Expect: Your Induced Lactation Timeline
Weeks 1-2: If using a medication protocol, breast changes such as tenderness or fullness may begin. If using a pumping-only approach, the priority is establishing a consistent pumping schedule, every two to three hours during the day, at least once at night.
Weeks 3-4: Pumping frequency increases. Some parents notice early drops of colostrum. Early colostrum at this stage indicates the stimulation protocol is taking effect.
Weeks 5-8: Milk production gradually increases. According to LLLI (2024), most parents with adequate information and support see measurable output by this stage. King Edward Memorial Hospital (Australia) recommends beginning the expressing phase six to eight weeks before the baby arrives for medication-based protocols.
After baby arrives: Breastfeed at the breast using a supplemental nursing system. Continue pumping between feeds. The combination of direct nursing and pumping sends the strongest signal to the body to increase production. Establishing consistent feeding and sleep patterns during this stage also supports overall routine.
Ongoing: Supply continues to build over weeks and months of consistent stimulation. Some parents see continued improvement for three to six months after beginning breastfeeding.
Setting realistic expectations matters. Most parents who induce lactation achieve a partial supply rather than exclusive breastfeeding. This is a success, not a shortfall. Partial breastfeeding still delivers antibodies, supports the infant's developing immune system, and provides the skin-to-skin contact that strengthens the parent-child bond.
As IBCLC Alyssa Schnell explains, "Because parents who haven't given birth do not have the hormones of pregnancy to get their bodies started with making milk, they need more information and support to make breastfeeding a reality" (LLLI).
What Is a Supplemental Nursing System (and How to Use One)?
A supplemental nursing system (SNS) is a device that delivers supplemental milk (formula or donor milk) through thin tubing taped alongside the nipple while the baby nurses at the breast. It solves the core challenge of induced lactation: the baby needs nutrition now, but the parent's supply is still building.

How a Supplemental Nursing System works
The benefit of an SNS is twofold. The baby receives adequate nutrition during each feeding, and the act of nursing at the breast simultaneously stimulates the parent's milk production. The baby's suckling is one of the strongest signals the body receives to increase supply.
Basic Setup:
Fill the SNS container with the appropriate amount of supplemental milk (formula or donor milk). Day one after birth, baby should be receiving 5-7ml per feed every 1-2 hours. Day 3 they should be receiving 22-27ml per feed. At week one, baby should be receiving 45-60ml per feed.
Thread the thin tubing along the breast so it sits slightly extended past the nipple
Position the baby at the breast so they latch onto both the nipple and the tubing
The baby draws supplement through the tubing while nursing
Two widely available brands are the Medela Supplemental Nursing System and the Lact-Aid Nursing Trainer. Both work on the same principle but differ slightly in design. Some parents also use nipple shields alongside an SNS to help with latch challenges.
SNS devices have a learning curve, but most parents find the setup becomes routine within the first several sessions. A certified lactation consultant can demonstrate correct positioning in a single consultation, which significantly reduces the adjustment period.
The Role of Professional Support
Induced lactation is not a process most parents can navigate alone. The right professional support significantly improves both outcomes and the day-to-day experience.
International Board Certified Lactation Consultant (IBCLC): An IBCLC is the gold standard for lactation support and the most important professional to have on your team during induced lactation. However, not all IBCLCs have experience with non-gestational lactation. When choosing a consultant, ask specifically about their experience with induced lactation protocols, and request references from non-gestational parents they have supported.
As IBCLC Jacob Engelsman notes, "Inducing lactation seems to be one of those things that many people don't hear about until after it's relevant to their life. I don't know how many times I've had someone shocked to learn it was an option" (Birthing Advocacy Doula Trainings).
Postpartum doula: A postpartum doula provides hands-on daily support with feeding logistics, emotional encouragement, and practical household help during the intensive early weeks. For parents inducing lactation, a doula can help manage the demanding pumping schedule, troubleshoot feeding challenges, and provide the consistent encouragement that makes a difference during the hardest days.
When to Seek Support:
Ideally, three to six months before the baby arrives, to plan the protocol and begin preparation
Intensively during the first two to four weeks after the baby arrives, when feeding logistics are most demanding
MissPoppins connects parents with certified virtual lactation consultants for private, 1:1 video sessions from home. For parents navigating induced lactation, an experienced IBCLC can review your protocol, demonstrate SNS technique, and adjust the plan as your supply develops, providing real-time clinical guidance throughout the process.
How to Get Started With Induced Lactation
Induced lactation involves multiple moving parts: medical guidance, equipment, scheduling, and emotional readiness. This checklist provides a concrete starting point for non-gestational parents considering the process.
Talk to your healthcare provider. Discuss your interest in induced lactation and ask about medication options. If your provider is unfamiliar with induced lactation protocols, request a referral to one who is, or consult an IBCLC with specific experience in this area.
Choose a protocol that fits your timeline. If you have six or more months before your baby arrives, the Newman-Goldfarb Regular Protocol offers the highest milk yield. Though speak with an IBCLC and your provider as certain medications are not safe for everyone. If your timeline is shorter, the Accelerated Protocol or a pumping-only approach may be more realistic. An IBCLC can help you decide.
Get your equipment ready. You will need a double electric breast pump (many insurance plans cover one at no cost), pump accessories, and storage bags or bottles. If you plan to use a supplemental nursing system, order it early so you can practice before the baby arrives. It's always a good idea to speak to an IBCLC prior to these purchases to ensure you get equipment that will meet your specific needs.
Build your support team. Schedule an initial consultation with an IBCLC experienced in induced lactation, ideally three to six months before the baby arrives. Consider adding a postpartum doula for hands-on support during the first weeks of breastfeeding.
Set realistic expectations. Partial breastfeeding is the most common outcome of induced lactation, and it is a meaningful success. Define what "success" looks like for your family before you begin as this reduces frustration and keeps the focus on bonding rather than volume.
Connect with community. Online groups and forums for non-gestational parents who have induced lactation can provide peer support, practical tips, and encouragement. La Leche League groups are one starting point.
Start a pumping log. Track your pumping sessions, duration, and output from day one. This data helps your IBCLC adjust your protocol and gives you a clear picture of progress over time.
Frequently Asked Questions About Induced Lactation
Can I breastfeed if I didn't give birth?
Yes. Induced lactation allows non-gestational parents to produce breast milk through breast stimulation, with or without medication protocols.
Is induced breast milk as nutritious as regular breast milk?
Research indicates that induced breast milk has comparable macronutrients to gestational breast milk (Delgado, 2023; PMC case report, 2024).
Can transgender women breastfeed?
Yes. Case studies confirm this, including a 2024 PMC case report and a 2021 case study by Wamboldt et al., both showing successful milk production with composition comparable to gestational breast milk.
Do I need a prescription to induce lactation?
Not necessarily. Pumping-only approaches require no medication. Medication-based protocols do require prescriptions, so discuss options with a healthcare provider experienced in induced lactation.
How much does induced lactation cost?
Costs vary by approach: a breast pump ranges from $0 with insurance to $200 or more out of pocket, IBCLC consultations with an IBCLC who specializes in induced lactation typically run $200 to $400 per session, and medication costs depend on the protocol and access method. Many insurance plans cover breast pumps and some lactation support. For a broader look at professional support pricing, see MissPoppins' guide to parent coaching costs.
Final Thoughts
Induced lactation is real, evidence-backed, and achievable with the right preparation and professional support. Whether a parent produces a full supply or supplements with formula or donor milk, any amount of breastfeeding provides immunological benefits and strengthens the bond between parent and child.
Every family's protocol, timeline, and definition of success will differ. Non-gestational parents who begin with an experienced IBCLC have a protocol, a troubleshooting partner, and a plan that can be adjusted as supply develops.
A certified lactation consultant with experience in induced lactation can help build a personalized plan, troubleshoot challenges in real time, and adjust the approach as supply develops. Talk to a certified lactation consultant on MissPoppins- private, certified, and available from home.